Legislation
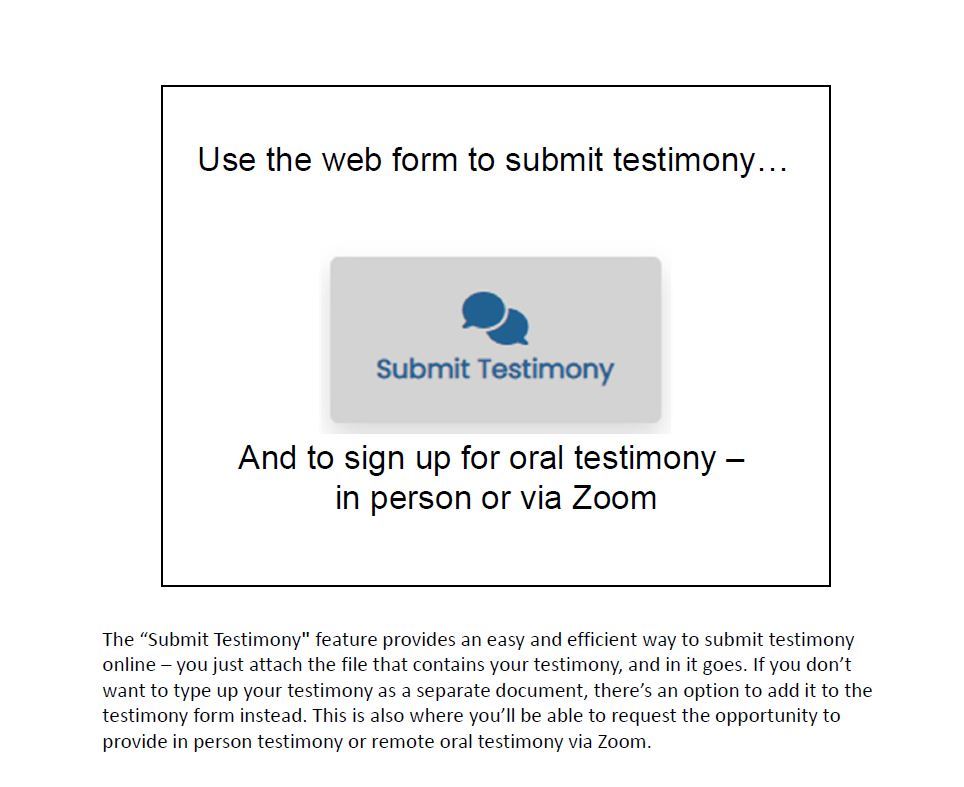
How to submit testimony:
Steps by Dr. Janet Boyd, DACM, DAc
credit to PAR for all images and text
---------------------------------------------------------------------------------------------------------------------
Please watch your member emails for updates so you can support the latest legislation for our profession!
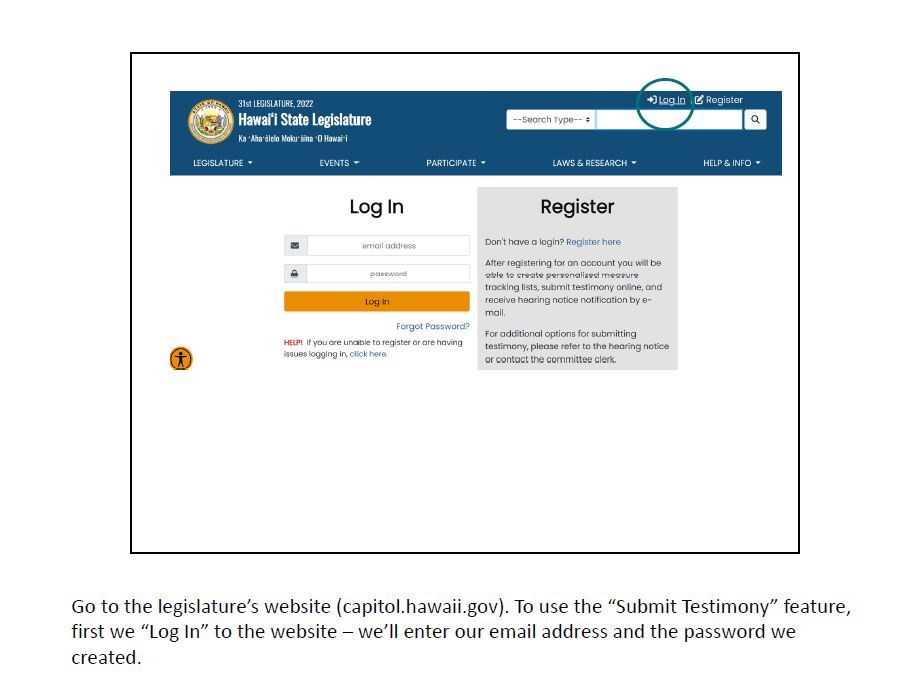
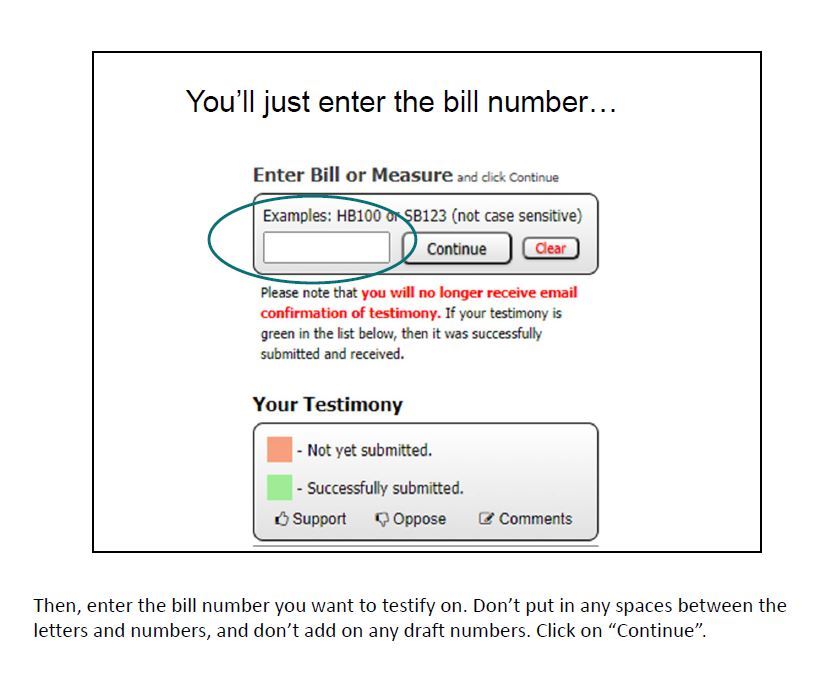
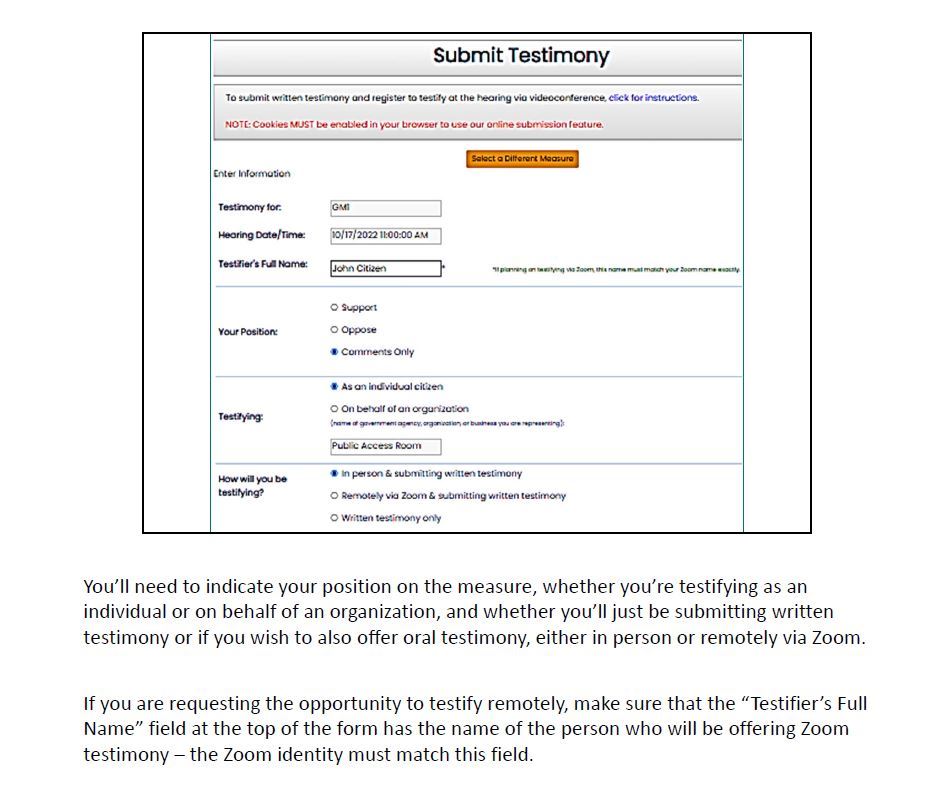
You can submit testimony up to 24 hours before a hearing at this link:
https://capitol.hawaii.gov/home.aspx

HAMA is closely monitoring legislation introduced in January 2020 by the Hawaii Physical Therapists Association that would allow "dry needling" to be added to the PT’s scope of practice in Hawaii. The Bills that have been introduced by their Association are HB 1807 and SB2225. "Dry needling" also known as trigger point acupuncture is a form of acupuncture called ashi acupuncture in which the points are located on tender spots reported by the patient. The AMA equivocated trigger point acupuncture with dry needling at the recent CPT code meeting. PTs use solid filiform needles to perform dry needling. Every solid filiform needle that enters the US is a Class II medical device that is classified by the FDA as an acupuncture needle. Dry needling is acupuncture. The latest scientific research shows that acupuncture is an effective intervention for patients with musculoskeletal pain and pain related to myofascial pain syndrome.
We, the acupuncturists of Hawaii, are strongly opposed to the inclusion of "dry needling" into the scope of practice for any practitioner that is not a licensed acupuncturist. This is a matter of public safety for the people of Hawaii.
In the statute of Physical Therapy 461J-2.5 HRS states: 461J-2.5 Prohibited practices. A physical therapist shall not use invasive procedures. For purposes of this reason, an invasive procedure is the breaking or puncturing of a person's good skin integrity, for example, through surgery or injections. Their new Bill has added more information to the legislature regarding this, that we, need to examine and have viable, truthful information why their course of legislative action would be a danger to public safety. Please read the following stances and current information on what is occurring right now, January 2020, on a national level, to understand and help you to form your testimony on this current situation.
ASA
Check out this fact sheet about acupuncture and dry needling from the American Society of Acupuncturists! Feel free to share it with colleagues, patients friends and any other supporters of acupuncture.
AAAOM
To find out more about what laws the national organization
NCCAOM
What is Dry Needling?
NCCAOM® Dry Needling Position Statement
“Dry needling” is acupuncture. Acupuncture is the insertion of thin solid needles into anatomical locations to treat disease, injury, pain, or dysfunction, and to promote health and wellness. “Dry needling” is a recently coined name for an acupuncture technique that involves the insertion of acupuncture needles directly into muscles and “trigger points” for the relief of musculoskeletal pain.
Licensed acupuncturists have practiced and documented this acupuncture technique, now referred to as “dry needling”, for decades in the US.
Some physical therapists and other healthcare providers have claimed that “dry needling” is “new” and “not acupuncture”, because the point locations and needling style are based on anatomical structures and physiological function rather than on traditional Chinese medicine acupuncture theory. In fact, licensed acupuncturists receive training in the application of both traditional foundations of acupuncture and modern biomedical theories and have done so since long before the term “dry needling” was invented.
“Dry needling” is an advanced and invasive procedure. In the hands of a practitioner who has received limited and/or substandard training, it has the potential to cause great harm. It can be considered safe only when performed by properly trained and experienced acupuncturists.
NCCAOM National Board-Certified AcupuncturistsTM receive hundreds of hours in the core skills required to correctly perform invasive and potentially dangerous needling techniques, assuring their competencies to insert and manipulate acupuncture needles safely.
Is there a required accredited academic program for the training of physical therapists to practice dry needling acupuncture?
There is no national standard entry-level academic curriculum that offers training or education in any form of needling for physical therapists. The only training in dry needling acupuncture for physical therapists are abbreviated continuing education workshops. There are no minimum hours or curriculum standards for these workshops.
Is there a valid and reliable examination to test competency of physical therapists in the practice of dry needling acupuncture?
No. There are no national psychometrically validated examinations to test competency of physical therapists in the practice of dry needling acupuncture.
What academic and clinical practice training are required for licensed
acupuncturists to practice dry needling acupuncture?
National Certification Commission for Acupuncture and Oriental Medicine
2025 M Street NW, Suite 800, Washington DC 20036 / (888) 381-1140 / info@thenccaom.org / www.nccaom.org
What is the NCCAOM?
-
The National Certification Commission for Acupuncture and Oriental Medicine (NCCAOM) is the only nationally accredited certification organization that assures entry-level competency of acupuncturists. The NCCAOM’s certification programs in Acupuncture and Oriental Medicine are accredited by a third- party accrediting body, National Commission for Certification Agencies (NCCA).
The NCCAOM’s mission is to assure the safety and well-being of the public and to advance the professional practice of acupuncture and Oriental medicine by establishing and promoting national evidence-based standards of competence and credentialing.
NCCAOM’s top priority is to protect the public from the unsafe practice of acupuncture and Oriental medicine by individuals who do not have appropriate training and meet competency standards.
What are the position statements of other professional organizations regarding the practice of “dry needling”?
Please follow these links:
American Academy of Medical Acupuncture Position Statement
American Academy of Physical Medicine and Rehabilitation Position Statement American Alliance for Professional Acupuncture Safety White Paper
American Association of Acupuncture and Oriental Medicine Position Statement American Medical Association Position Statement
American Society of Acupuncturists Position Statement
American Traditional Chinese Medical Association Paper on Dry Needling Council of Colleges of Acupuncture and Oriental Medicine Position Paper
The Center for Medicare & Medicaid Service Announcement:
Please pay attention to the definitions # 2 and #4, for it relates to Dry Needling:
January 22, 2020
Dear Colleagues, Patients, and Supporters of Acupuncture:
On Tuesday, January 21st the Centers for Medicare and Medicaid Services (CMS) announced the historic decision to not only cover acupuncture for low back pain, but also to go out of their way to include Licensed Acupuncturists as the key group of providers for acupuncture services, along with physicians. This unprecedented support of a licensure group who is not currently a part of Medicare, as well as the endorsement of our academic system, speaks to the care and trust they put in us, and the desire for Medicare beneficiaries to receive the best care possible. Please, recognize how phenomenal these actions are, and, if you choose to contact CMS, thank them.
Many providers are unclear as to why supervision is indicated and why the term “auxiliary personnel” is used. The answers to these questions are simple: CMS is only empowered to approve independent care for provider groups who are already within Medicare via the Social Security Act. Their options are to exclude the group, or find a way to include practitioners such as Licensed Acupuncturists with supervision by a provider within the structure of CMS. This is neither a slight to the profession, nor an error in any way. Provider types outside of Medicare are by CMS definition “auxiliary personnel”. Auxiliary personnel must be supervised by Medicare providers. This is the maximal freedom that can be granted until the Social Security Act is amended to include LAcs, by an act of Congress. The power to do that does not lie with CMS, but with our profession.
Many questions naturally arise from this transformation in non-pharmacologic care for chronic low back pain for Medicare beneficiaries. How will the care be billed? How will payment be arranged? What type of supervision is required? How many units can be billed in a single session? Can we use electrical stimulation? The answers to these questions must remain forthcoming at present, as many of the procedural components of this have not yet been developed by CMS itself, and many clarifications are needed.
What we do know about this new expansion of care is the following:
-
Up to 20 visits will be allowed per year, with 12 visits in the first 90 days with demonstration of improvement. This is both a generous allotment, and truly allows a fair trial of acupuncture.
-
Only a physician as defined by Medicare in 1861(r)(1) (i.e. an MD or DO), and those with “a masters or doctoral level degree in acupuncture or Oriental Medicine from a school accredited by the Accreditation Commission on Acupuncture and Oriental Medicine (ACAOM)” may furnish acupuncture. This clearly prevents those with substandard training from providing services, protecting the quality of care for beneficiaries.
-
The type of supervision required was changed at the request of the LAc profession from “direct” to “the appropriate level”. This accommodation adds tremendous latitude for collaborative agreements between LAcs and MD/DO providers, nurse practitioners, clinical nurse specialists, and physician assistants, allowing the maximum freedom within CMS’ power. While nurse practitioners, clinical nurse specialists, and physician assistants may not practice acupuncture, their supervisory availability also vastly expands the potential for collaborative agreements. It is implicit in this that these providers are not specifically directing the nature of the acupuncture treatment, but rather are collaboratively assuring patient diagnoses, safety, follow-up, and connection to the established care system.
4. Dry Needling is clearly defined as a “type of acupuncture” within the determination. For a full read of the CMS decision, please see the CMS Decision Memo.
The American Society of Acupuncturists and the NCCAOM are proud to stand among those many groups lending support and high-level information to CMS towards their determination.
American Society of Acupuncturists
National Certification Commission for Acupuncture and Oriental Medicine
|
|


Follow us on Facebook
![]()
Address:
Hawaii Acupuncture Medicine Association PO Box 104 Kamuela, HI 96743 | Email: a 501(c)6 non-profit organization | *Please note: Website ADA Compliance updates are in progress |